


Onychomycosis is a disease that affects the nails. In children, this disease may be self-limited or may extend to a contiguous nail. Symptoms include nail thinning, longitudinal ridging, and onycholysis. Diagnosis is usually based on history and clinical appearance, but a skin biopsy is necessary for confirmation. Histologic findings also support the diagnosis.
Dermatitic lesions


The cutaneous manifestations of dermatophytosis are characterized by the presence of keratinized debris. The infection can involve the nail or other cutaneous structures. The fungi are known to survive on human scales for up to 12 months. The classification of dermatophytosis includes infections affecting the nail apparatus or hair follicles.
The skin lesions may be pink or light brown and may be absent in nontanned individuals. Lesions may merge and cover an extensive geographical area. They may also occur on the neck, upper arms, or axillae. The affected areas may be a source of contact with creams and other topical agents. The diagnosis of this disease is made based on the symptoms and the underlying condition.
The fungi responsible for onychomycosis can cause many different types of skin and nail infections. Some types are more common in children and teens, while others are more severe in adults. The fungi that cause onychomycosis are categorized into three main genera, which include Trichophyton rubrum, trichophyton, and epidermophyton. In the United States, T. rubrum is the most common cause of epidermal dermatophytosis in the adult population. Some species are worldwide, while others are endemic to one or more continents. A specific type of dermatophytosis is tinea capitis, tinea favosa, and tinea unguium.
Symptomatic dermatophytosis may appear as small ulcers, crusts, or intertrigo, and may involve the entire nail apparatus. Onychomycosis can lead to chronic paronychia and total nail dystrophy. Additionally, persistent candidiasis may be characterized by crusts, erosions, and warty hyperkeratoses.
Sporotrichoid nodules
A billable/specific ICD-10-CM code for sporotrichosis nodules in nail onychomycosis is B35.9. It is used to indicate the diagnosis for reimbursement purposes. The causative fungi are Microsporum, trichophyton, and epidermophyton. In addition, specific types of dermatophytoses are included in the diagnosis, including tinea capitis, fvosa, and unguium, ringworm of the nails. A red rash is an asymptomatic symptom of ringworm infection; however, this does not mean that the patient has ringworm.
Mycobacterial furunculosis
ICD-10 code A31.9 is used to indicate a diagnosis for reimbursement purposes. This diagnosis code may differ from the version used in other countries. Nontuberculous mycobacteria that can cause this infection include Kansasii, Marinum, Scrofulaceum, and Flavescens. Nontuberculous mycobacteria are commonly called m. Gordonae, m. Abuse, and m. Duvall.
Nail involvement


There are several treatments for onychomycosis that target the fungal infection in the nail plate. The most common treatment options include oral and topical antifungal agents. Topical agents are difficult to apply to the nail plate because of low adherence rates. Systemic agents are more effective but are associated with a higher risk of systemic side effects. Noninvasive laser therapy may be the next step in onychomycosis treatment.
There are several ways to code this condition in your medical records. The most common way to code it is B35.1. This code indicates a diagnosis for reimbursement purposes. This specific code is only required when the date of service is after October 1, 2015.
In some cases, it may be necessary to take nail clippings for periodic acid-Schiff staining and histologic examination. Depending on the severity of the problem, the nail may be discoloured or thickened. If the infection progresses, the skin under the nail may become inflamed and painful. Additionally, white patches may develop on the nailbed and scaly skin next to it. Finally, people with this condition may suffer from psychosocial problems because of the appearance of their nails.
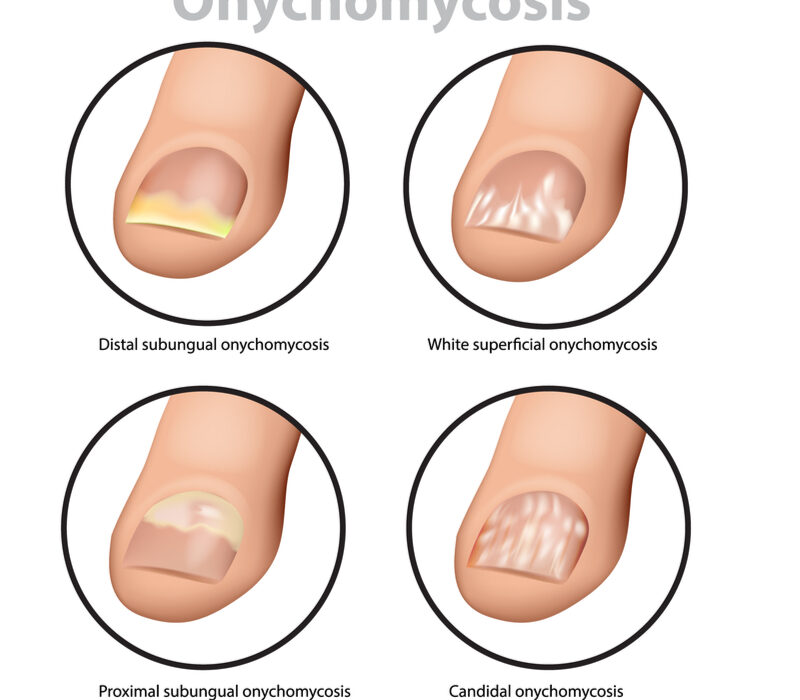
Onychomycosis may also present with symptoms such as onycholysis. A white granular appearance is indicative of a fungal infection of the nail. Yellow spots may appear in the lunula and proximal nail fold. Onycholysis also occurs in psoriasis. There are several types of onychomycosis.
Topical antifungal drugs are commonly prescribed for onychomycosis. These medications contain ciclopiroxolamine, a synthetic hydroxypyridine. This medication does not affect sterol biosynthesis but instead inhibits the enzymes responsible for the production of toxic peroxides in the fungal cell. The study concluded that cicllopirox 8 percent lacquer led to a 17.4% cure rate after 24 weeks and a 42% cure rate after 48 weeks. The treatment also has side effects and is associated with hepatotoxicity.
Nail involvement in onychomycoasis is very common and affects ten percent of the population. Patients with recurrent tinea pedis may have onychomycosis as a subclinical form. However, recurrent infection can predispose a person to lower extremity cellulitis. This fungus is commonly found on the fingers, toenails, and toenails and is caused by dermatophytes and yeasts.